When people hear the word dementia, they often think of it as a single disease. In reality, dementia is not one condition — it’s an umbrella term for over 100 different disorders that affect the brain. (Continued below video…)
A helpful comparison is cancer. Just as cancer includes many diseases with different progressions, stages, and treatments, dementia also includes multiple types — each with distinct causes, symptoms, and care needs.
Memory loss connects them all.
But the early warning signs differ, and recognizing those differences can significantly affect treatment options and long-term planning.
Below are the four most common types of dementia and what distinguishes each one.
1. Alzheimer’s Disease (60–80% of cases)
Alzheimer’s disease is the most common form of dementia, accounting for roughly 60–80% of cases, depending on the population studied.
Early Signs
Alzheimer’s typically begins with short-term memory loss.
A person may:
- Clearly remember childhood events
- Struggle to recall a recent conversation
- Repeat the same story multiple times without realizing it
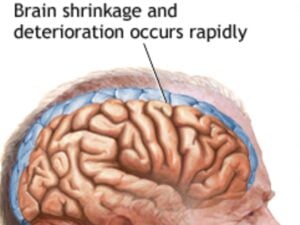
What’s Happening in the Brain?
The disease often begins in the hippocampus, a small seahorse-shaped structure responsible for forming new memories. When this region is affected, older memories remain intact longer, but new ones fail to “stick.”
Progression
Alzheimer’s is usually slow and gradual.
People often live 8–10 years after diagnosis, making early planning especially important.
2. Vascular Dementia
Vascular dementia is the second most common type. Unlike Alzheimer’s, it is caused by reduced blood flow to the brain.
Causes May Include:
- Stroke
- Small vessel disease
- Multiple small infarcts (“mini-strokes”)
When blood supply decreases, brain cells die in the affected areas.
Early Signs
Memory loss may or may not appear first.
Instead, the earliest problems often involve executive functioning:
- Difficulty organizing tasks
- Trouble with decision-making
- Losing the ability to follow multi-step processes
A classic example:
Someone who has made the same Sunday roast for 30 years suddenly:
- Leaves the stove on
- Forgets ingredients
- Skips important steps
They know what they want to do — but can’t organize how to do it.
Brain Area Affected
The cerebral cortex, particularly areas involved in executive control and planning.
Symptoms may fluctuate rather than steadily decline.
3. Lewy Body Dementia
Lewy body dementia is less widely understood but still relatively common.
It is caused by abnormal deposits of a protein called alpha-synuclein in the brain. It is biologically related to Parkinson’s disease dementia.
Early Signs
- Visual hallucinations
- Severe sleep disturbances
- Motor problems (similar to Parkinson’s)
- Fluctuating clarity — some days alert, other days confused
Memory loss may occur, but it is not always the first symptom.
Brain Area Affected
The brainstem is often involved early. This region controls automatic functions like:
- Sleep
- Breathing
- Walking
Because of this, sleep disruption and movement difficulties are common.
One hallmark feature is fluctuation:
Some days the person seems relatively fine. Other days, reality feels distorted.
4. Frontotemporal Dementia (FTD)
Frontotemporal dementia often appears earlier than other types — sometimes in people in their 40s or 50s.
It is one of the most challenging forms because memory loss is not the first symptom.
Early Signs
- Personality changes
- Behavioral shifts
- Loss of social filter
- Language difficulties (in some variants)
Someone who was once diplomatic may become blunt or socially inappropriate.
This isn’t intentional — it reflects brain changes.
Brain Areas Affected
The frontal lobe and/or temporal lobe.
There are two main variants:
- Behavioral variant FTD – personality and judgment changes
- Language variant FTD – speech and word-finding difficulties
Memory problems typically emerge later in the disease course.
Is Dementia Different for Men and Women?
Yes.
Women are disproportionately affected, particularly by Alzheimer’s disease.
For years, researchers assumed this was simply because women live longer. But emerging evidence suggests biological factors may play a role:
- Hormonal changes
- Menopause
- Differences in brain structure and physiology
An important nuance:
Women often perform better on verbal fluency tests, which are commonly used in cognitive screening. As a result, symptoms may be masked longer — leading to later diagnosis.
Women are also more likely to serve as caregivers, increasing overall burden.
Treatments: Do They Differ by Type?
Yes — and this is why correct diagnosis matters.
Currently:
- No dementia can be cured.
- Most cannot be reversed.
- Treatments focus on slowing progression and managing symptoms.
Example: Alzheimer’s-Specific Therapy
A new class of drugs, including lecanemab, has been approved in some regions for early Alzheimer’s disease.
Important:
- It is only for Alzheimer’s — not other dementias.
- It must be given in early stages or during mild cognitive impairment.
Other Treatment Approaches
- Physical therapy (especially in Lewy body dementia)
- Occupational therapy
- Cognitive rehabilitation
- Behavioral therapy
- Cardiovascular risk management (for vascular dementia)
Because each dementia affects different brain systems, supportive therapies differ accordingly.
The Key Takeaway
All dementias involve cognitive decline.
But they are not the same disease.
The earliest symptoms can point to:
- The underlying biology
- The affected brain region
- The most appropriate treatments
- The right support strategy
If you or someone you love is experiencing changes in memory, behavior, sleep, or executive function — speak with a healthcare provider. Early identification can meaningfully change the care pathway.
Visual Comparison: The Four Most Common Types of Dementia
| Feature | Alzheimer’s Disease | Vascular Dementia | Lewy Body Dementia | Frontotemporal Dementia (FTD) |
|---|---|---|---|---|
| % of Cases | 60–80% of dementias | 10–20% (varies) | 5–10% (often underdiagnosed) | ~5–10% (more common under 65) |
| Typical Age of Onset | 65+ | 65+ (can follow stroke at any age) | 60+ | 40s–60s |
| First Brain Area Affected | Hippocampus | Varies (often cerebral cortex) | Brainstem & cortex | Frontal and/or temporal lobes |
| Primary Early Symptom | Short-term memory loss | Executive dysfunction (planning, organizing) | Visual hallucinations, fluctuating cognition | Personality or behavior change |
| Memory at Onset | Impaired early | May be intact initially | May fluctuate | Often intact early |
| Hallucinations | Rare early | Rare | Common, especially visual | Rare early |
| Motor Symptoms | Late stage | Sometimes (if stroke-related) | Early Parkinson-like symptoms | Usually later |
| Progression Pattern | Slow, gradual decline | Stepwise or fluctuating | Fluctuating day-to-day | Gradual but behaviorally dramatic |
| Classic Real-Life Example | Repeats same story, forgets recent conversation | Knows what to cook but forgets steps | Sees people who aren’t there, severe sleep disruption | Becomes socially inappropriate or unusually blunt |
| Underlying Cause | Amyloid & tau protein buildup | Reduced blood flow / strokes | Alpha-synuclein protein deposits | Frontal/temporal neuron degeneration |
| Treatment Considerations | Some disease-modifying drugs (early stage only) | Manage vascular risk factors | Symptom-specific therapy; caution with some meds | Behavioral management, speech therapy |
| Care Planning Emphasis | Long-term cognitive decline | Cardiovascular control | Safety due to hallucinations & motor risk | Behavioral support & family education |
Quick Clinical Pattern Recognition
If the first symptom is memory, think:
→ Alzheimer’s
If the first symptom is difficulty organizing tasks, think:
→ Vascular dementia
If the first symptom is hallucinations or major sleep disturbance, think:
→ Lewy body dementia
If the first symptom is personality change, think:
→ Frontotemporal dementia