Cochrane's Leqembi Ruling Used Dr. Andrews' Bar "Inappropriately"
COCHRANE SERIES, PART 3 - DEEP DIVE: False alarm. The Cochrane Review shook confidence in Leqembi. It rests on a…
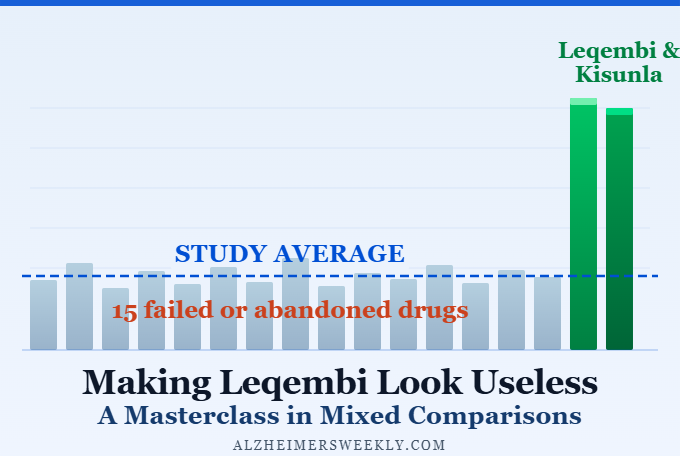
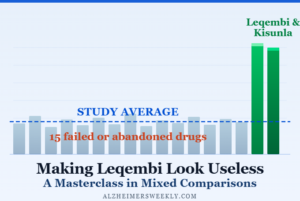
Making Leqembi Look Useless: A Masterclass in Mixed Comparisons
COCHRANE SERIES, PART 2 - HOW IT HAPPENED: A new review just went viral in the media, declaring Alzheimer's drugs…
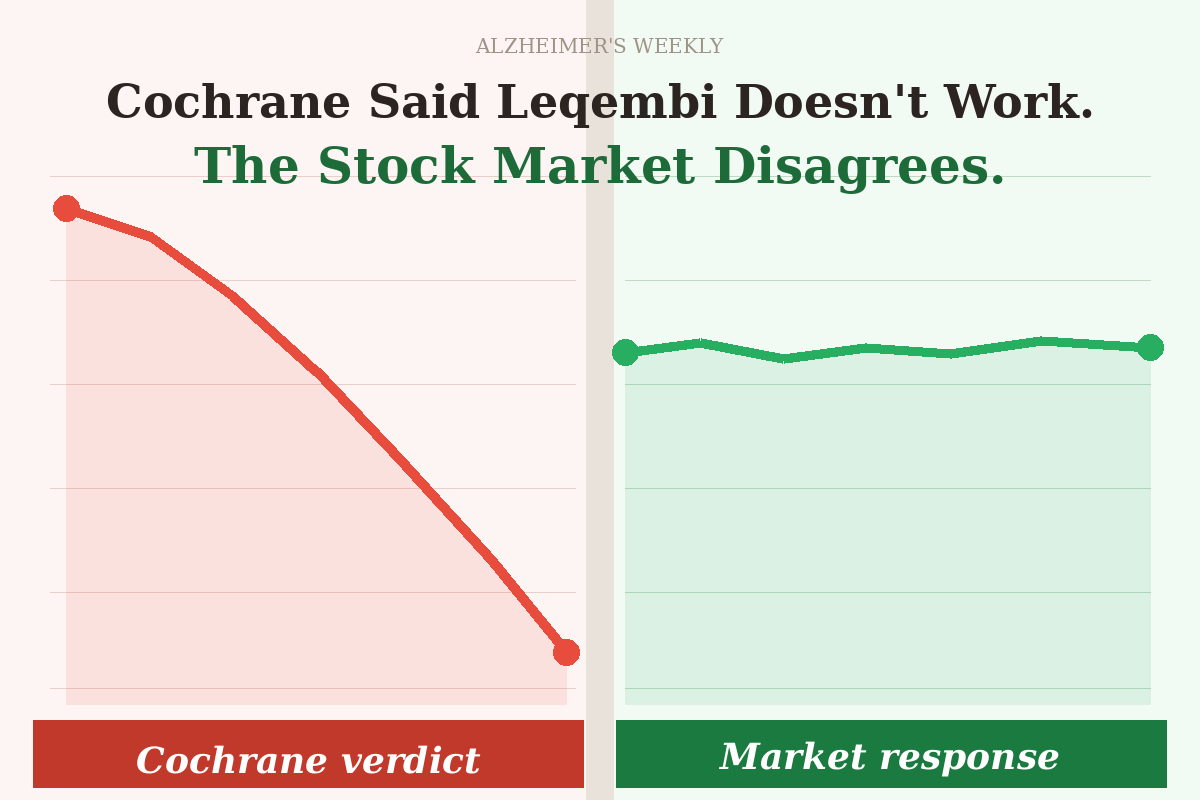
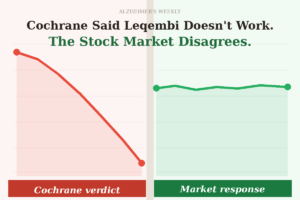
Cochrane Said Leqembi Doesn't Work. Why Didn't Anyone Seem to Care?
COCHRANE SERIES, PART 1 - WHAT HAPPENED: A respected review called a breakthrough Alzheimer's drug useless. Experts shrugged. Investors, who…

Beyond Leqembi: Can a New RNA Deal Advance Alzheimer’s Care?
In a new deal with Alloy Therapeutics, Biogen—the makers of Leqembi—is investing in RNA technology that could point toward what…

A Simpler Leqembi? New Alteogen Deal Could Make Injections Faster, Easier
Could Leqembi be given faster and more easily in the future? The new Biogen–Alteogen deal suggests it’s possible—but it doesn’t…

Leqembi’s Real Advantage Isn’t the Drug — It’s the Network
The diagnostic and treatment network behind Leqembi may be its biggest competitive edge.

Why Leqembi Works: Fc Activates the Brain’s Cleanup Crew
New research reveals that Leqembi’s Fc region switches on microglia — the brain’s immune cells — helping them clear toxic…

How Doctors Decide Who Qualifies for Leqembi
Many diagnosed patients won’t qualify — here are the 7 medical criteria.
What 400 Alzheimer’s Patients Gained From Leqembi and Kisunla
In a one-hour seminar, a leading neurologist answers the most important questions families ask about what these new therapies can…

Leqembi Prescriptions Could Rise Sharply. Why?
Alzheimer’s treatment eligibility may be far larger than previously thought. A major Nature study using blood tests suggests millions more…
Leqembi: Slowing Alzheimer’s — What You Need to Know
Leqembi is one of the first Alzheimer’s treatments proven to slow decline. A new MRI study helps explain what it…

New At-Home Leqembi: What It Means for Alzheimer's
IMAGINE THIS: Instead of going to an infusion center for treatment, you can switch to a weekly injection at home.…

3-Minute 'Fastball' Alzheimer’s Test Could Speed Access to Leqembi
Access to Leqembi, the new Alzheimer’s drug, has been slowed by lengthy diagnoses. The “Fastball” brainwave test could change that…
Leqembi and Kisunla: Inside the Infusion Experience
They’re not just pills—they’re precision infusions designed to slow Alzheimer’s at its source. See UCLA’s cutting-edge Amyloid Immunotherapy Care Program,…

"Is Leqembi Worth It?" Costs and the Road to Wider Access
Leqembi, the first Alzheimer's-modifying drug, is a giant step forward—but how many people are getting it, and what does it…

How Many Leqembi Patients Are There?
Alzheimer's rates are on the rise. How is today's best treatment, Leqembi (generic lecanemab) doing in the fight against it?

Leqembi Best at Fighting Alzheimer's in Men
See why Leqembi is even more effective in males than females, at fighting Alzheimer's.
Leqembi Becomes Europe's First Alzheimer's Antibody
The European Union authorizes Leqembi as its very first Alzheimer's drug to target an underlying cause of Alzheimer's.

Leqembi & Kisunla: Extending Independent Living
A new analysis of the benefits of these Alzheimer's treatments scores the days and ways patients succeed in living independently.

Leqembi: Europe Checks It's Safety; U.S. Approves Monthly Doses
The EMA has announced its schedule for reviewing the Alzheimer's drug Leqembi (lecanemab) for use in Europe. Meanwhile, the U.S.…

Is Leqembi Shrinking the Alzheimer's or the Brain?
Leqembi and Kisunla are the new Alzheimer's immunotherapies. A loss of brain volume associated with these immunotherapies may be caused…

Catching Up to America: Europe Recommends Leqembi® for Alzheimer's
The European Medicines Agency (EMA) recommended approving Leqembi® (generic lecanemab) for Alzheimer's. Originally skeptics, learn how the "Clarity AD" trial…

Leqembi Autoinjector to Treat Alzheimer's in Seconds, Not Hours
Leqembi is an FDA-Approved Alzheimer's treatment. Hospital infusions take an hour each. 2025 is looking to see a new 15-second…

3 Questions on Leqembi & Kisunla, the New Alzheimer's Drugs
The 2 newest Alzheimer's drugs, Leqembi (lecanemab) and Kisunla (donanemab) show promise, but many questions remain. Here are the three…

Leqembi: Pioneering Alzheimer’s Drug Faces Challenge in Europe
While the initial headlines might seem discouraging, there’s always more to the story. 🌟

How to Choose Between Kisunla vs. Leqembi, The New Alzheimer's Drugs
The newest Alzheimer's drugs, Kisunla and Leqembi, are the first to actually slow down Alzheimer's. How do they compare to…

Leqembi Launched in China to Fight Alzheimer's
China is the third country to launch LEQEMBI for sale, to fight Alzheimer's, following the United States and Japan.

Making it Easier to Take Leqembi for Alzheimer's
A drug for Alzheimer’s, called Leqembi, might soon be given less often. Right now, patients get it through a drip…

What Treats Alzheimer's Better? Leqembi or a Plant Based Diet?
Dr. Dean Ornish publishes the first trial investigating plant-based diets fighting or reversing early-stage Alzheimer's. The results are eye-opening.

LEQEMBI® for Alzheimer’s Now in USA, China, Japan, South Korea
South Korea joined other countries in approving LEQEMBI® (generic lecanemab) for mild cognitive impairment, mild and early Alzheimer's. Learn how…