
Vascular Dementia and Vascular Cognitive Impairment
Vascular dementia and vascular cognitive impairment (VCI) are caused by injuries to the vessels supplying blood to the brain. These disorders can be caused by brain damage from multiple strokes or any injury to the small vessels carrying blood to the brain. Dementia risk can be significant even when individuals have suffered only small strokes.
Amazon Books & Videos
about Alzheimer’s and Dementia:
FREE Newsletter:
Vascular dementia and VCI arise as a result of risk factors that similarly increase the risk for cerebrovascular disease (stroke), including atrial fibrillation, hypertension, diabetes, and high cholesterol. Vascular dementia also has been associated with a condition called amyloid angiopathy, in which amyloid plaques accumulate in the blood-vessel walls, causing them to break down and rupture. Symptoms of vascular dementia and VCI can begin suddenly and progress or subside during one’s lifetime.
Some types of vascular dementia include:
1. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL).
This inherited form of cardiovascular disease results in a thickening of the walls of small- and medium-sized blood vessels, eventually stemming the flow of blood to the brain. It is associated with mutations of a specific gene called Notch3, which gives instructions to a protein on the surface of the smooth muscle cells that surround blood vessels. CADASIL is associated with multi-infarct dementia, stroke, migraine with aura (migraine preceded by visual symptoms), and mood disorders. The first symptoms can appear in people between ages 20 and 40. Many people with CADASIL are undiagnosed. People with first-degree relatives who have CADASIL can be tested for genetic mutations to the Notch3 gene to determine their own risk of developing CADASIL.
2. Multi-infarct dementia.
This type of dementia occurs when a person has had many small strokes that damage brain cells. One side of the body may be disproportionally affected, and multi-infarct dementia may impair language or other functions, depending on the region of the brain that is affected. Doctors call these “local” or “focal” symptoms, as opposed to the “global” symptoms seen in AD that tend to affect several functions and both sides of the body. When the strokes occur on both sides of the brain, however, dementia is more likely than when stroke occurs on one side of the brain. In some cases, a single stroke can damage the brain enough to cause dementia. This so-called single-infarct dementia is more common when stroke affects the left side of the brain—where speech centers are located—and/or when it involves the hippocampus, the part of the brain that is vital for memory.
Subcortical vascular dementia, also called Binswanger’s disease. This is a rare form of dementia that involves extensive microscopic damage to the small blood vessels and nerve fibers that make up white matter, the “network” part of the brain believed to be critical for relaying messages between regions. The symptoms of Binswanger’s are related to the disruption of subcortical neural circuits involving short-term memory, organization, mood, attention, decisionmaking, and appropriate behavior. A characteristic feature of this disease is psychomotor slowness, such as an increase in the time it takes for a person to think of a letter and then write it on a piece of paper.
Other symptoms include urinary incontinence that is unrelated to a urinary tract condition, trouble walking, clumsiness, slowness, lack of facial expression, and speech difficulties. Symptoms tend to begin after age 60, and they progress in a stepwise manner. People with subcortical vascular disease often have high blood pressure, a history of stroke, or evidence of disease of the large blood vessels in the neck or heart valves. Treatment is aimed at preventing additional strokes and may include drugs to control blood pressure.
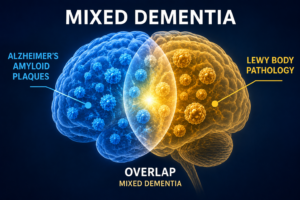
3. Mixed Dementia
Researchers are still working to understand how underlying disease processes in mixed dementia influence each other. It is not clear, for example, if symptoms are likely to be worse when a person has brain changes reflecting multiple types of dementia. Nor do we know if a person with multiple dementias can benefit from treating one type, for example, when a person with AD controls high blood pressure and other vascular disease risk factors.










My husband Rip.💖, passed away February 8th, 2018, in 2014 he was diagnosed with normal pressure hydrocephalus,before that he got agitated and thru something at me, never in the 50 years we were married, he ever raise a hand to me😕 he had brain surgery and vp shunt inserted into the brain and stomach on the left side of the stomach, then 2015, diagnosed with vascular dementia 😕 he was sometimes have short term memory loss, agitation, scared, cried, and woukd say i want a divorce, was that normal behavior with vascular dementia, he had hypertension, diabetes, and was a heart patient too 2008 had 3 stents. No one dr, neurologist explain to me,what to expect 😢
My husband had the same history as Thu Feb 19 (comments) until 2009 aged 71 when he suffered his first major stroke -no dementia at that time –it wasn't until his 3rd stroke this year that VD was mentioned and no information given at that time as to the prognosis. He also worked with asbestos.
My husband at the age of 56 was diagnosed with vascular dementia he was in the navy and worked with asbesto. Do you think asbesto has any connection with vascular dementia? Please help ! Thanks
My husband has a long history of atrial fibrillation. He is on blood thinners but no treatment to regulate his heart rate has even been successful. 6 years ago at age 67 he was diagnosed with vascular dementia (VD). I have long thought the source of his VD might be the irregular heart rate and resulting lack of effective oxygenation of his brain. No health professional has had a strong opinion about this possibility.