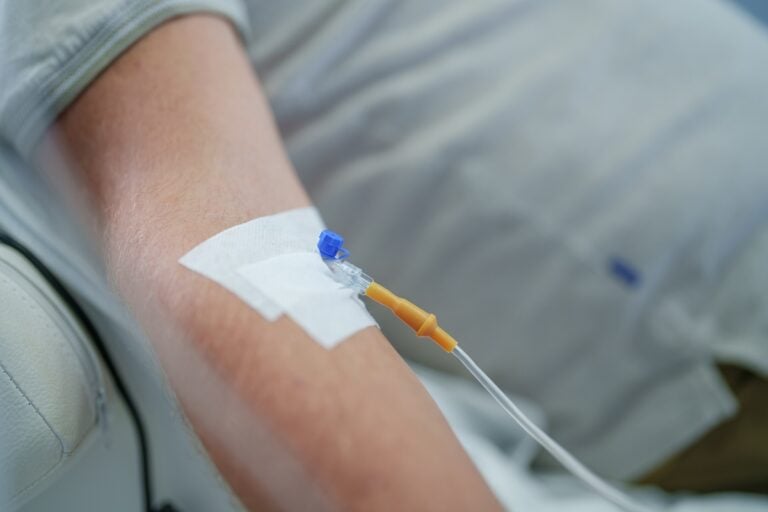
People beginning treatment with Leqembi have traditionally needed to visit an infusion center every two weeks. For patients and caregivers, that can mean recurring travel, scheduling difficulties, and long hours spent receiving treatment.
The U.S. Food and Drug Administration has now approved an at-home injection option that allows eligible patients to begin Leqembi treatment outside an infusion center.
The medication can be administered by the patient or by a caregiver who has received appropriate training. The change may make treatment more accessible, especially for people who live far from specialist medical centers or rely on family members for transportation.
What the FDA approved
Leqembi, also known by its generic name lecanemab, is a disease-modifying Alzheimer’s treatment developed by Eisai and Biogen.
The new approval allows eligible patients to begin treatment using a subcutaneous injection administered under the skin. Previously, patients generally began treatment through intravenous infusions at a medical facility.
The home injection is designed to deliver the same active medication in a more convenient form. It does not represent a new Alzheimer’s drug or a different treatment strategy.
The main change is how the medication is delivered.
Where the injection can be given
Patients or caregivers may administer the injection in several approved areas of the body:
- Abdomen: At least two inches away from the belly button. This may be the easiest location for many patients who inject themselves.
- Thighs: Into the front or middle-outer portion of the thigh.
- Upper arms: Into the outer back portion of the upper arm. This location should be used only when a caregiver or healthcare professional administers the injection.
Patients and caregivers should receive detailed instruction from the treating medical team before attempting an injection at home.
Injection sites may need to be rotated to reduce irritation. The medication should not be injected into skin that is tender, bruised, red, hardened, scarred, or otherwise damaged.

Why at-home treatment matters
Leqembi requires repeated doses over an extended period. Even when a treatment is medically appropriate, the practical burden can make it difficult for families to begin or continue therapy.
Regular infusion appointments may require:
- Transportation to a specialty center.
- Time away from work for caregivers.
- Coordination with other medical appointments.
- Long waits before, during, and after an infusion.
- Additional difficulty for people living in rural areas.
Allowing patients to receive the medication at home could reduce some of those burdens.
For caregivers, the change may provide greater scheduling flexibility. For patients, it may mean fewer disruptions and less time spent traveling to medical facilities.
However, at-home administration does not mean that Leqembi has become a simple or routine treatment. It remains a specialized Alzheimer’s therapy requiring careful patient selection and continuing medical oversight.
Who may receive Leqembi
Leqembi is approved for people in the early stages of Alzheimer’s disease.
This generally includes people with:
- Mild cognitive impairment caused by Alzheimer’s disease.
- Mild Alzheimer’s dementia.
- Confirmed evidence of amyloid plaques in the brain.
Leqembi has not been approved for people with moderate or severe Alzheimer’s dementia.
Before beginning treatment, patients typically undergo testing to confirm that Alzheimer’s-related amyloid is present. Doctors must also evaluate the patient’s overall health, medications, genetic risk factors, and possible vulnerability to treatment complications.
Leqembi slows decline
Leqembi is designed to remove amyloid-beta plaques from the brain. These abnormal protein deposits are one of the defining biological features of Alzheimer’s disease.
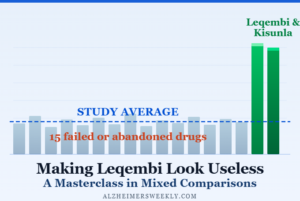
In a large clinical trial, people receiving Leqembi experienced a slower rate of cognitive and functional decline than those receiving a placebo.
(The treatment slowed decline by approximately 27% over 18 months on the study’s primary clinical measure.)
That result was statistically significant, but it does not mean that patients improved or regained abilities already lost to Alzheimer’s disease.
Leqembi does not cure Alzheimer’s. It may modestly slow progression in appropriately selected patients who are treated during the early stages of the disease.
Safety monitoring remains essential
The convenience of home injections does not eliminate the treatment’s risks.
Leqembi can cause amyloid-related imaging abnormalities, commonly called ARIA. These abnormalities may involve swelling in the brain or small areas of bleeding.
Many cases cause no noticeable symptoms and are discovered only on MRI scans. In other cases, patients may experience:
- Headache.
- Confusion.
- Dizziness.
- Vision changes.
- Nausea.
- Difficulty walking.
- Seizures or other neurological symptoms.
Rare cases can be serious or life-threatening.
Patients still need MRI scans before and during treatment. Their doctors may also recommend additional monitoring depending on their symptoms, medical history, genetic profile, or use of blood-thinning medications.
Families should immediately report new neurological symptoms to the treating medical team.
What this means for caregivers
For caregivers, the new option could make Leqembi treatment significantly easier to manage.
Home administration may reduce travel, missed work, and the strain of organizing repeated infusion appointments. It may also allow treatment to fit more naturally into a patient’s daily routine.
Before taking responsibility for an injection, caregivers should make sure they understand:
- How to store and prepare the medication.
- How to select and rotate injection sites.
- How to administer the full dose correctly.
- How to dispose of used injection equipment safely.
- Which injection reactions are expected.
- Which symptoms require immediate medical attention.
Caregivers should not treat the home injection as a replacement for medical follow-up. Regular appointments, MRI monitoring, laboratory testing, and communication with the Alzheimer’s treatment team remain necessary.
A practical advance rather than a new breakthrough
The FDA approval does not make Leqembi more effective, and it does not remove the drug’s medical risks.
What it may do is make treatment more practical.
For some families, the ability to begin therapy at home could remove a major obstacle to accessing a disease-modifying Alzheimer’s treatment. It may be particularly valuable for patients who live far from infusion centers or whose caregivers struggle to manage frequent clinic visits.
The decision represents an important step toward making Alzheimer’s treatments easier to deliver. Whether it substantially expands access will also depend on insurance coverage, medication costs, caregiver training, specialist availability, and the ability of medical systems to provide appropriate safety monitoring.