A Verdict That Shook the Room
Leqembi (Generic name: lecanemab) arrived on the market with hard-won credibility. Regulators in more than 50 countries had reviewed the evidence and approved it. Neurologists had begun prescribing it. Families had built plans around it.
Then last week’s Cochrane review landed with the force of a verdict. Seventeen clinical trials. More than 20,000 participants. One damning conclusion: anti-amyloid drugs produce effects that are way below the minimal effect necessary to be noticeable at all for patients and caregivers.
But there is a significant problem at the center of that conclusion. And it comes from the very scientist whose research the Cochrane team used to support it.
The Yardstick the Review Relied On
To declare Leqembi’s benefit undetectable, the Cochrane review needed a measuring standard — a threshold defining the smallest change in cognitive function that a patient or caregiver would actually notice in daily life. That standard is called the Minimal Clinically Important Difference, or MCID.
The most widely cited source for the MCID in Alzheimer’s trials is a 2019 study led by Dr. Scott Andrews, then a researcher at Eli Lilly. His team found that a change of roughly 1 to 2 points on the CDR-SB — the 18-point cognitive scale used in Leqembi’s clinical trial — was the minimum associated with a noticeable difference in a patient’s abilities.
Leqembi’s trial produced a difference of 0.45 points versus placebo. Well below the Andrews threshold. The Cochrane review used that gap to conclude the drug’s benefit was clinically meaningless.
So far, so straightforward. Except for one thing.
The Author of That Study Says It Was Misapplied
Dr. Andrews has been explicit and public about this. In a widely noted webinar following Leqembi’s approval, he stated directly that his findings had been “misapplied” to discount the drug’s benefits. Applying his analysis to require a 1-point difference between treatment groups, he said, “sets up unrealistic expectations for these emerging therapies” — and was “inappropriate.”
More significantly, Dr. Andrews and his co-authors published a formal response in a peer-reviewed journal making the same point in precise scientific language. They stated that their findings “have often been misinterpreted or misapplied,” and clarified that their MCID estimates should be used to measure meaningful change within an individual patient over time — not to judge the difference between two groups in a clinical trial.
That distinction is not a minor technicality. It is the entire argument.
Why the Distinction Matters
The Andrews threshold was built by asking: how much does an individual patient need to decline before they or their caregiver notices a difference in daily life? That is a within-patient question — tracking one person over time.
Leqembi’s trial reports something different: the average difference between two groups of patients — those who received the drug and those who received a placebo — over 18 months. That is a between-group question.
These are not the same measurement. Applying a within-patient threshold to a between-group result is, in Dr. Andrews’ own word, inappropriate. And the consequences of that misapplication are significant. Reaching a 1 to 2 point MCID in an 18-month trial would require nearly halting Alzheimer’s progression entirely — since the placebo group itself only declined by around 1.5 to 1.7 points over that same period. The bar the Cochrane review used would disqualify virtually any drug that didn’t essentially cure the disease outright.
What Leqembi’s Numbers Actually Show
When the same trial data is framed correctly, the picture changes. Rather than asking whether 0.45 points is noticeable at 18 months, researchers translated the finding into real-world time.
A slope analysis of the trial data showed that Leqembi-treated patients needed 25.5 months to reach the same level of decline that placebo patients reached at 18 months — a difference of roughly 7.5 months of preserved function. Research focused specifically on daily independence found that for a patient with early-stage disease, Leqembi extended the ability to manage medications, handle finances, and perform routine tasks by approximately 10 months.
That is not a number that appears anywhere in the Cochrane review’s framing of the evidence.
What a Rigorous Review Should Have Done
Scientific consistency requires engaging with counterevidence. The Cochrane team cited the Andrews MCID threshold as support for their central conclusion. A consistent review would also have engaged with Dr. Andrews’ formal, published clarification that his threshold was never designed for this application.
It did not. The review’s conclusion — that Leqembi’s effects are unnoticeable to patients and caregivers — rests on a standard its own primary source has publicly and explicitly said should not be used this way.
What This Means for Caregivers
This does not mean Leqembi is a miracle drug. It is not. Its benefits are real but modest, its risks are genuine, and access remains uneven depending on where you live.
What it does mean is this: the Cochrane review’s most alarming claim — that patients and caregivers would not notice any difference — is built on a methodological foundation that the scientific community has already challenged, including the researcher whose work anchors it.
If you were on a path toward Leqembi before last week, the Cochrane review has not given you a scientific reason to abandon it. It has given you a reason to understand more carefully how evidence gets interpreted — and misinterpreted — on the way from a clinical trial to a headline.
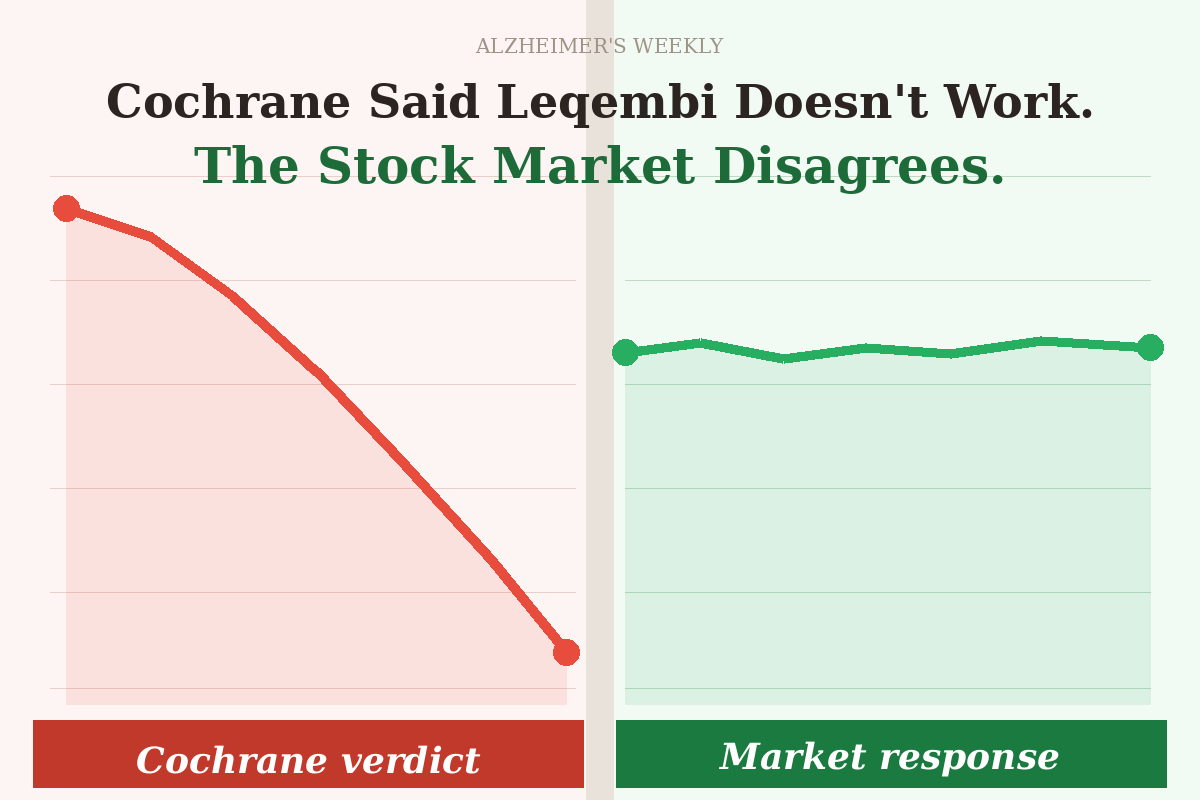
This is the third and most detailed installment in our Cochrane Series. If you’re just arriving here, Cochrane Said Leqembi Doesn’t Work. The Stock Market Disagrees. is the place to start — it explains the headline, the reaction, and what it means for families right now. From there, Making Leqembi Look Useless: A Masterclass in Mixed Comparisons walks through the core methodological flaw. Together, the three pieces tell the full story of a study that made more noise than its evidence warranted.
As always, if you have questions, leave them in the comments — we read every one.
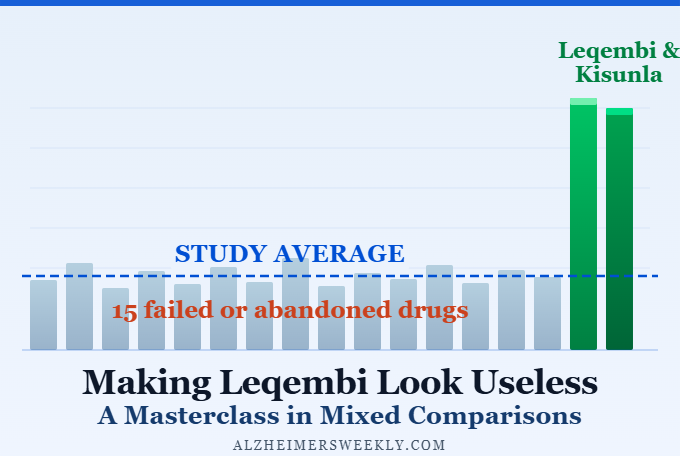
Making Leqembi Look Useless: A Masterclass in Mixed Comparisons
Cochrane Said Leqembi Doesn't Work. Why Didn't Anyone Seem to Care?

Beyond Leqembi: Can a New RNA Deal Advance Alzheimer’s Care?