
Drugs widely prescribed to the elderly could be responsible for a decline in cognitive and physical function according to research from the University of East Anglia and the Regenstrief Institute. (Continued below video…)
A key report reveals that anti-cholinergic drugs — which are used to treat conditions including asthma, high blood pressure, insomnia, dizziness and diarrhea — could impact physical functions in elderly patients such as eating and getting dressed.
Up to half the UK’s elderly population are prescribed at least one medication with anti-cholinergic properties. Other anti-cholinergic drugs are also sold over the counter without the need for a prescription.
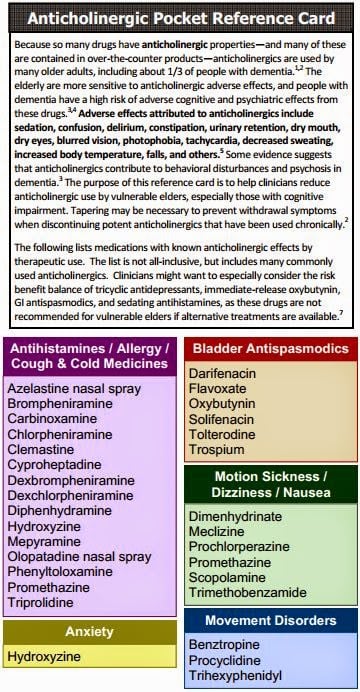
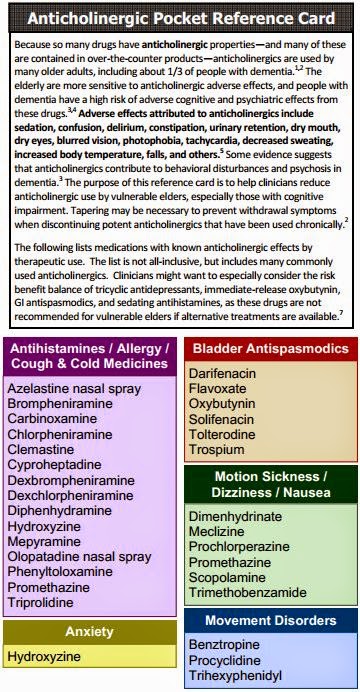
These medications affect the brain by blocking a key neurotransmitter called acetylcholine. But they have been associated with side effects including dizziness, sedation, confusion, delirium, constipation and blurred vision.
Previous studies have shown a link between these drugs and cognitive impairment, but this study is the first to summarise evidence of a physical decline among the elderly.
The research team looked at 46 studies from around the world that included 60,944 patients who had taken anti-cholinergic medications for up to 10 years.
Lead researcher Dr. Chris Fox, from UEA’s Norwich Medical School, said. “We examined the effect of anti-cholinergic medication on physical function over a large time frame spanning decades of research.
“This is the first research to show a significant decline in physical, as well as cognitive, function. This means patients could become less and less able to carry out everyday activities like walking around, feeding themselves, washing and getting dressed.
“This is likely due to the direct effect on cholinergic neurons compounded by an increase in the blood-brain permeability.
“We have also seen that the type of anti-cholinergic drug may be important, and more research needs to be done to ascertain which types are more dangerous than others.
“Further studies are also needed to establish whether the cognitive decline is definitely induced by these medications — or the whether the diseases for which they are prescribed are a factor too.
“In the meantime, the prescription of these medications for people with dementia should be cautiously assessed, monitored and attempts made to reduce the burden whenever feasible. Clinicians should conduct regular reviews of the medication taken by their older patients, both prescribed and over the counter, and wherever possible avoid prescribing multiple drugs with anti-cholinergic effects.”
The international research team included experts from the Regenstrief Institute and the Indiana University Center for Aging Research in the US, Aston University, the University of Aberdeen and the Norfolk and Norwich University Hospital in the UK.
Co-author Dr Noll Campbell, from the Regenstrief Institute, IU Center for Aging Research and Purdue University College of Pharmacy, said: “Anticholinergics, both over-the-counter and prescription medications, impact the lives of older adults in ways doctors, patients and their families may not realize.
“I don’t see use of these medications declining. Doctors and patients are familiar with these drugs and unfortunately are far less familiar with equally effective alternatives.”
Dr Campbell advises that rather than taking sleeping pills with anti-cholinergic properties, one could refrain from napping, limit evening exercise and remove distractions from the bedroom. Meanwhile hospitals and nursing homes could work to keep older adults awake and stimulated during the day, naturally encouraging night-time slumber.
Stands on Shoulder of Earlier Study
An earlier study a few years prior also linked a significantly increased risk for developing dementia, including Alzheimer’s disease, to taking commonly used medications with anticholinergic effects. This was especially true when the drugs were taken at higher doses or for a longer time. Many older people take these medications, which include nonprescription diphenhydramine (Benadryl).
JAMA Internal Medicine published the report, called “Cumulative Use of Strong Anticholinergic Medications and Incident Dementia.”
The study used more rigorous methods, longer follow-up (more than seven years), and better assessment of medication use via pharmacy records (including substantial nonprescription use) to confirm this previously reported link.
First Study
It is the first study to show a dose response: linking more risk for developing dementia to higher use of anticholinergic medications. And it is also the first to suggest that dementia risk linked to anticholinergic medications may persist — and may not be reversible even years after people stop taking these drugs.
“Older adults should be aware that many medications — including some available without a prescription, such as over-the-counter sleep aids — have strong anticholinergic effects,” said Shelly Gray, PharmD, MS, the first author of the report, which tracks nearly 3,500 Group Health seniors participating in the long-running Adult Changes in Thought (ACT), a joint Group Health-University of Washington (UW) study funded by the National Institute on Aging. “And they should tell their health care providers about all their over-the-counter use,” she added.
Review Drugs Regularly
“But of course, no one should stop taking any therapy without consulting their health care provider,” said Dr. Gray, who is a professor, the vice chair of curriculum and instruction, and director of the geriatric pharmacy program at the UW School of Pharmacy. “Health care providers should regularly review their older patients’ drug regimens — including over-the-counter medications — to look for chances to use fewer anticholinergic medications at lower doses.”
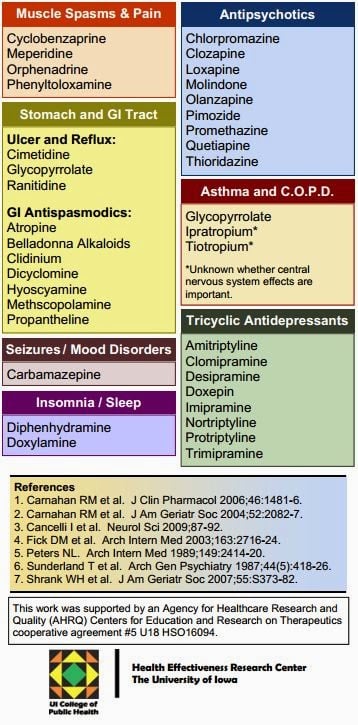
For instance, the most commonly used medications in the study were
- Tricyclic antidepressants like doxepin (Sinequan)
- First-generation antihistamines like chlorpheniramine (Chlor-Trimeton)
- Antimuscarinics for bladder control like oxybutynin (Ditropan)
The study estimated that people taking at least 10 mg/day of doxepin, 4 mg/day of chlorpheniramine, or 5 mg/day of oxybutynin for more than three years would be at greater risk for developing dementia.
Alternatives
Dr. Gray said substitutes are available for the first two:
- A selective serotonin re-uptake inhibitor (SSRI) like citalopram (Celexa) or fluoxitene (Prozac) for depression
- A second-generation antihistamine like loratadine (Claritin) for allergies
It’s harder to find alternative medications for urinary incontinence, but some behavioral changes can reduce this problem.
“If providers need to prescribe a medication with anticholinergic effects because it is the best therapy for their patient,” Dr. Gray said, “they should use the lowest effective dose, monitor the therapy regularly to ensure it’s working, and stop the therapy if it’s ineffective.”

Anticholinergic effects happen because some medications block the neurotransmitter called acetylcholine in the brain and body, she explained. That can cause many side effects, including:
- drowsiness,
- constipation,
- retaining urine,
- dry mouth and eyes.
Thousands of People in ACT Study
“With detailed information on thousands of patients for many years, the ACT study is a living laboratory for exploring risk factors for conditions like dementia,” said Dr. Gray’s coauthor Eric B. Larson, MD, MPH. “This latest study is a prime example of that work and has important implications for people taking medications — and for those prescribing medications for older patients.” Dr. Larson is the ACT principal investigator, vice president for research at Group Health, and executive director of Group Health Research Institute (GHRI). He is also a clinical professor of medicine at the UW School of Medicine and of health services at the UW School of Public Health.
Some ACT participants agree to have their brains autopsied after they die. That will make it possible to follow up this research by examining whether participants who took anticholinergic medications have more Alzheimer’s-related pathology in their br










Could you provide rhe above reference cards to neurologists so they could give them to their patients? I’ve had to do my own research for this information, it should be provided to all caregivers of dementia patients.
If you click the reference card within the article, it should cause the card to open up in a fresh window. There, it should be easy to print. Then it can be easily given out in the way you described. Hope this helps.
Mirtazapine (Remeron) is also anticholinergic: https://www.health.harvard.edu/mind-and-mood/two-types-of-drugs-you-may-want-to-avoid-for-the-sake-of-your-brain